Authors: Emily Thompson, DO and Michael Galuska, MD
ABSTRACT
A 44–year-old male construction worker presented to the ED with right radial wrist pain. Physical exam findings were consistent with De Quervain’s Tenosynovitis (DQT) and bedside ultrasound of the first extensor compartment of the wrist confirmed the diagnosis, showing edema within the tendon sheath of the extensor pollicis brevis tendon (Image 1).
CASE PRESENTATION
A 44-year-old male construction worker presented to the emergency department with chief complaint of right radial wrist pain after most recently doing work with a jackhammer on a bridge. He was found to have a positive Finkelstein test on physical exam, as well as swelling over the radial side of the wrist. There was also pain with ulnar deviation of the wrist. Bedside ultrasound was utilized (Image 1) to assist in diagnosing DQT. The image of the extensor pollicis brevis (EPB) tendon shows notable edema within the tendon sheath. He was treated with a thumb spica splint and pain control with 60mg of IM ketorolac while in the department. He was given a prescription for oral naproxen and referred to hand surgery for outpatient follow up.
DISCUSSION
De Quervain’s Tenosynovitis (DQT) is a common condition causing pain in the extensor compartment of the forearm, frequently diagnosed in patients presenting with a history that includes repetitive hand motions involving extension or supination of the wrist or closing and unclosing of the fist.1 The exact etiology of the condition is unknown but is believed to involve microtrauma to the dorso-radial tendons, most specifically the first dorsal compartment tendons, the extensor pollicis brevis (EPB) and abductor pollicis longus (APL) resulting in inflammation and thickening of the tendons.2,3 DQT can be diagnosed on examination using Finkelstein Test and utilizing bedside soft tissue ultrasound. Finkelstein test is performed by requesting that the patient create a fist with the affected hand, then perform ulnar deviation. Reproduction of the pain with this mechanism will support the diagnosis of DQT.1 Diagnosis can also be made with ultrasound which has been shown to have 96.3% sensitivity and a 93.3% specificity for DQT. 4 This disease is common in pregnant women, hence the common descriptor “mother’s disease”, and is also known to frequently present in video game enthusiasts, earning the term “gamer’s thumb”. 3 It is more than twice as common in women (affecting 1.3%) than men (0.5%). 1
First line treatment for DQT is non-operative and includes immobilization with a thumb spica splint, non-steroidal anti-inflammatories, and steroid injections. Outpatient referral to a hand specialist is recommended if patients fail initial conservative therapy.3
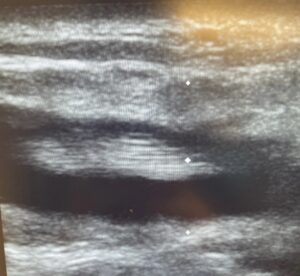
Image 1: Longitudinal US of the EPB Tendon within Dorsal Radial Compartment of Wrist
REFERENCES
[1] Allbrook, Victoria. “‘The side of my wrist hurts’:’De Quervain’s tenosynovitis’.” Australian Journal of General Practice 48.11 (2019): 753-756. doi: 10.31128/AJGP-07-19-5018
[2] Shehab, Ramsey, and Mark H. Mirabelli. “Evaluation and diagnosis of wrist pain: a case-based approach.” American Family Physician 87.8 (2013): 568-573.
[3] Currie, Kelly Bettina, Kashyap Komarraju Tadisina, and Susan E. Mackinnon. “Common Hand Conditions: A Review.” JAMA 327.24 (2022): 2434-2445. doi:10.1001/jama.2022.8481
[4] Lee, Kwang-Hyun, et al. “Ultrasonographic evaluation of the first extensor compartment of the wrist in de Quervain’s disease.” Journal of Orthopaedic Science 19.1 (2014): 49-54. doi: 10.1007/s00776-013-0481-3