Peter Nesbitt, OMS-IV @LECOM, Erie, PA
Dhimitri Nikolla, DO @AHN Saint Vincent Hospital, Erie, PA
CASE
60 year-old male with quadriplegia due to spinal cord injury and chronic Foley catheter presented to the emergency department (ED) with hematuria and confusion. The catheter was exchanged one day prior to ED presentation. The abdominal and genitourinary exams were normal except gross hematuria in the urine bag. His vital signs were normal. Lab results included a lactic acid of 3.4 mg/dL, white blood cell (WBC) count of 11 x109/L with 34% bandemia, and creatinine of 0.54 mg/dL. A urinalysis revealed 3+ blood, positive nitrite, 3+ leukocyte esterase, and too-numerous-to-count red blood cells and WBCs.
He was treated for severe sepsis due to urinary tract infection (UTI) with 30ml/kg of normal saline and piperacillin/tazobactam in the ED. He was admitted on cefepime; however, a few hours later, a rapid response was called due to hypotension. A triple lumen central line was placed and vasopressors were started. A bedside ultrasound showed bilateral hydronephrosis and a distended bladder concerning for Foley catheter misplacement (Figure 1). A stat computed tomography (CT) scan of his abdomen and pelvis was obtained (Figure 2).

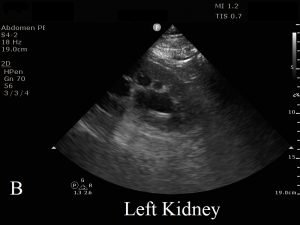

Figure 1 displays images from the patient’s bedside point of care ultrasound showing bilateral hydronephrosis (A,B) and a distended bladder without visualization of the Foley balloon (C).
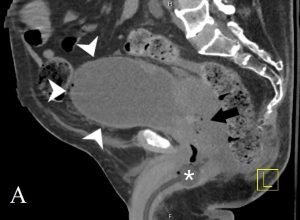

Figure 2 displays sagittal (A) and coronal (B) images of the patient’s CT abdomen and pelvis showing the misplaced Foley catheter in the prostate (white asterisk), periprostatic gas (black arrow), and distended bladder (white arrowheads) (A) as well as bilateral hydronephrosis (black arrow heads) (B).
DIAGNOSIS & DISCUSSION
Septic shock due to a urinary tract infection complicated by a urinary obstruction due to a misplaced Foley catheter
Urinary tract infections (UTI) are the most frequent infection in patients with past or acute spinal cord injury, and placement of a urethral catheter can increase the daily incidence of bacteriuria by 3-10%.1,2 However, Foley placement can often be difficult in quadriplegic patients and may result in urinary obstruction if misplaced.3 As high as 10.5% of patients with septic shock due to UTI can have an associated urinary obstruction, and those with an associated urinary obstruction have a 16.1% higher mortality compared to those without, 27.3% vs 11.2%, respectively.4 Therefore, early evaluation for urinary obstruction in patients with septic shock from UTI should be considered.
CASE CONCLUSION
The misplaced Foley catheter was removed and large clots were pulled from the urethral meatus. A coude tip urinary catheter was placed on first attempt with bedside ultrasound confirmation of the catheter in the bladder (Figure 3). The patient improved quickly. Urine cultures grew Pseudomonas aeruginosa and Serratia marcescens both sensitive to cefepime. He was discharged 7 days later.

Figure 3 displays the urinary catheter balloon (white arrow) in the bladder.
TEACHING POINTS
- UTI is the most common cause of infection in patients with spinal cord injury.
- In patients with septic shock from a urinary source, an obstructive process must be considered and evaluated.
- Point of care bedside ultrasound is a quick and easy way to evaluate for appropriate Foley placement and urinary obstruction.
REFERENCES
- Salameh A, Mohajer MA, Daroucihe RO. Prevention of urinary tract infections in patients with spinal cord injury. CMAJ. 2015;187(11):807–811.
- Brusch JL. Urinary Tract Infections in Spinal Cord Injury. Medscape. https://emedicine.medscape.com/article/2040171-overview#a1. Accessed: July 19, 2019.
- Vaidyanathan S, Singh G, Hughes PL, Soni BM. Acute Urinary Obstruction in a Tetraplegic Patient from Misplacement of Catheter in Urethra. Clin Med Insights Case Rep. 2016;9:1–4.
- Reyner K, Heffner AC, Karvetski CH. Urinary obstruction is an important complicating factor in patients with septic shock due to urinary infection. Am J Emerg Med. 2016 Apr;34(4):694-6.